Our success rates
(based on data from 2024)
All our patients, and prospective patients, enter treatment hoping for a successful outcome. Choosing a clinic to support you on your journey can be a difficult decision.
We know that patients will use the success rates of various clinics to help inform their decision and we therefore try to be as open as possible about the data we present. What you should bear in mind is that our individual clinic success rates cannot tell you how likely you are to have a baby. There are so many variable factors involved and a consultation with a doctor as your initial appointment can help to provide you with some extra clarity taking all of your personal circumstances into account.
What is included in, or excluded from, our data?
The data in this information leaflet is all based on the same sample of treatments. The sample does not include any patients using donor eggs, or those who have used any form of pre-implantation genetic testing (such as PGT-A, PGT-M, PGT-SR). It includes treatments where donor sperm has been used. Below we explain why these groups are excluded.
The age of the egg at the time of collection can impact on the success of the treatment. Female fertility will continue to decrease every year, whether or not someone is healthy and fit, because the number and quality of the eggs decreases with age. Current professional guidelines state that eggs should not be taken from donors aged 36 or over. In 2024 the average age of egg donors used in treatment in our Clinic was 28. As a result, we have removed treatment cycles using donor eggs from this data. This gives you a truer representation of the treatment success rates for people in your age category using eggs of the same age as yours, as it would otherwise give a misleading impression of higher success rates.
The Human Fertilisation and Embryology Authority (HFEA) classes PGT-A (pre-implantation genetic testing for aneuploidy) as a treatment add-on. This means that there is not enough evidence to show that it is effective at improving the chances of having a baby for most fertility patients. Whilst PGT-A does not carry any additional known risks for the person undergoing fertility treatment, it is known to carry some risks for the embryo. As a result of the existing scientific uncertainties, and unless otherwise clinically indicated, PGT-A is not routinely used in treatment for everyone at our Clinic. This is why cases where we have performed PGT-A are excluded from the general data presented in this leaflet, as it would otherwise give a misleading impression of higher success rates.
If you have specific questions regarding treatments using donor eggs or PGT you should ask for a consultation with a member of our clinical team.
How are the results calculated?
We know that choosing a fertility clinic is a big decision. Looking at success rates can help, but it’s important to remember that these numbers can’t predict your personal chances of having a baby. Everyone is different, and many things can affect the outcome of treatment.
This leaflet provides an overview of our IVF success rates, based on a variety of treatment types. To ensure the results are as accurate and meaningful as possible, we present data for patients using their own eggs separately from those who used donor eggs or had preimplantation genetic testing (PGT-A), as these groups often have different outcomes.
Our success rates include treatments with both partner and donor sperm.
At your first consultation, our doctors will look at your health and history to give you a more
personal idea of your chances.
What Metrics Do We Use?
We use a few different ways to show success:
- Positive pregnancy test: A result you can get with a urine or blood test.
- Clinical pregnancy: This is when we see a heartbeat on an early scan, usually between 6 and 9 weeks of pregnancy.
- Per embryo transfer: This means we count each time an embryo was transferred.
- Per embryo transferred: This means we count each embryo that was transferred, not just the full procedure.
We also track:
- Early pregnancy loss: How often a pregnancy doesn’t reach the stage of a visible heartbeat.
- Multiple pregnancy rate: How often more than one baby starts growing at once.
Our team follows national advice to reduce the chance of twins or triplets, as they carry more risks for both the parent and babies. We’ll guide you on how many embryos should be transferred to keep you safe while giving you the best chance of success.
Our Fresh Transfers
Fresh embryo transfers use embryos that haven’t been frozen and they normally take place 5 or 6 days after the egg collection.


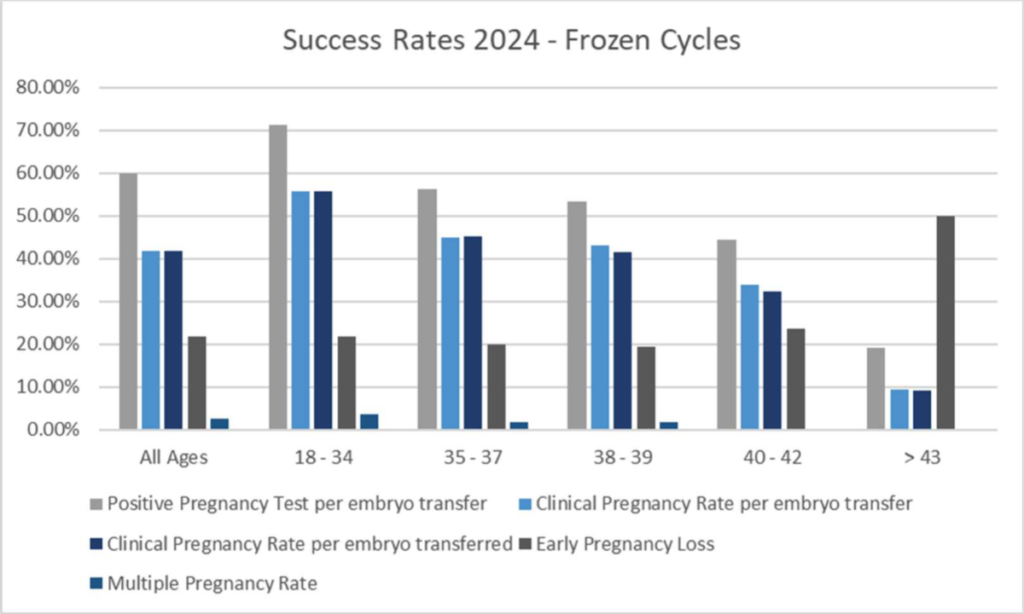
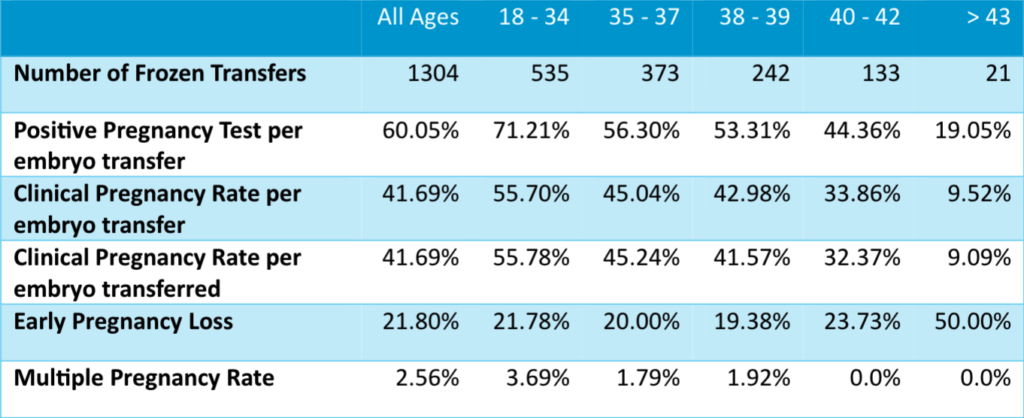
Our Frozen Transfers
Any embryos remaining after treatment can be frozen and transferred at a later stage.
This data is still calculated based on the age of the egg at the time it was collected and then frozen – not at the age the patient was when they had the transfer.
Live births
Our aim is always to help you bring home a healthy baby.
We ask patients to update us after giving birth, but not everyone does. If we don’t hear back, we can’t include that birth in the data, which makes the numbers slightly less accurate.
Here are the live birth rates (per embryo transferred) after a fresh embryo transfer: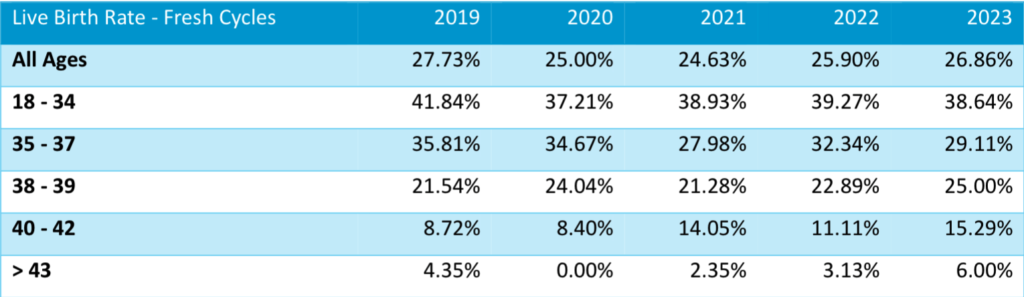
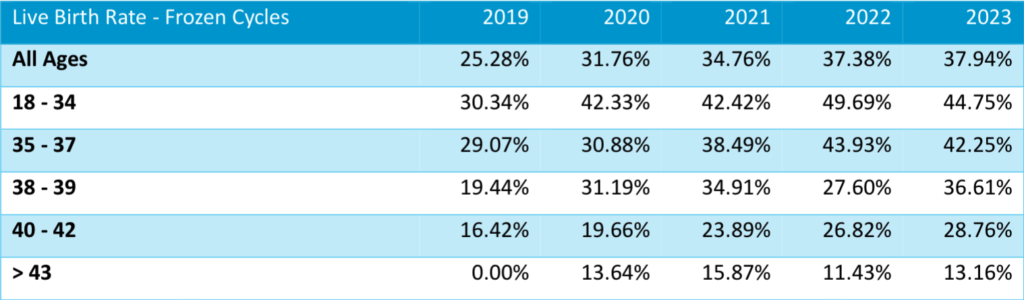
Here are the live birth rates (per embryo transferred) after a frozen embryo transfer:
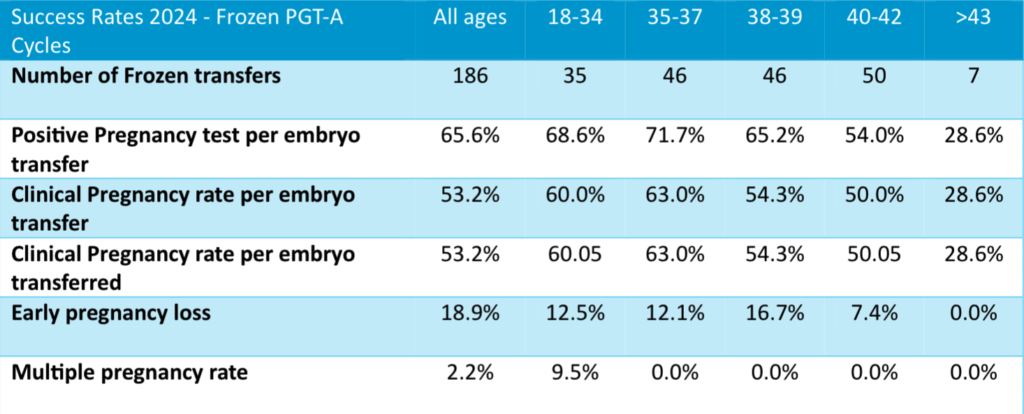
Treatments involving PGT-A
PGT–A (Pre–implantation Genetic Testing for Aneuploidy) checks embryos for chromosome number changes in the embryo for better embryo selection. This is not offered to everyone and is only used when needed.
When we do PGT-A, embryos must be frozen while we wait for the results. These transfers are always done in frozen cycles.
Treatments involving Donor Eggs
People who use donor eggs often have different results, as egg donors are usually younger than a typical patient.
In 2024, our donors were 28 years old on average. Here’s how treatments with donor eggs (no PGT-A) performed.
The number of treatments we do is small and therefore it is not broken down into age groups.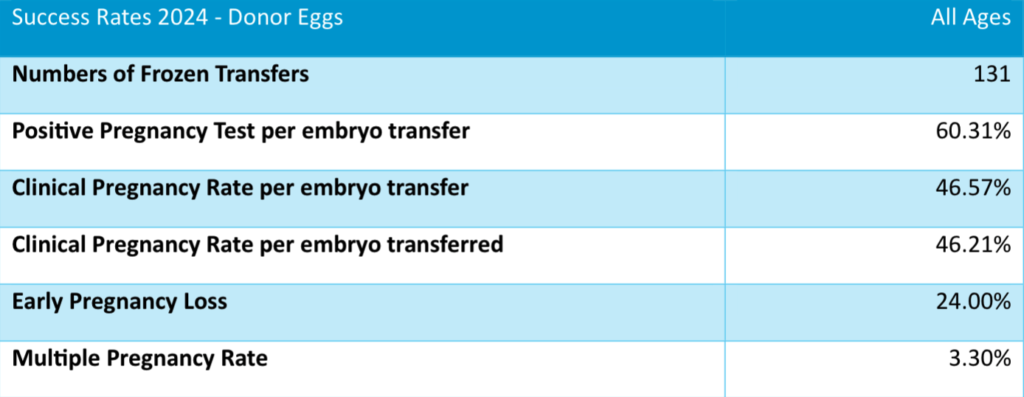
If you want to know whether using donor eggs in your treatment might be more beneficial for you, please speak to one of our doctors.
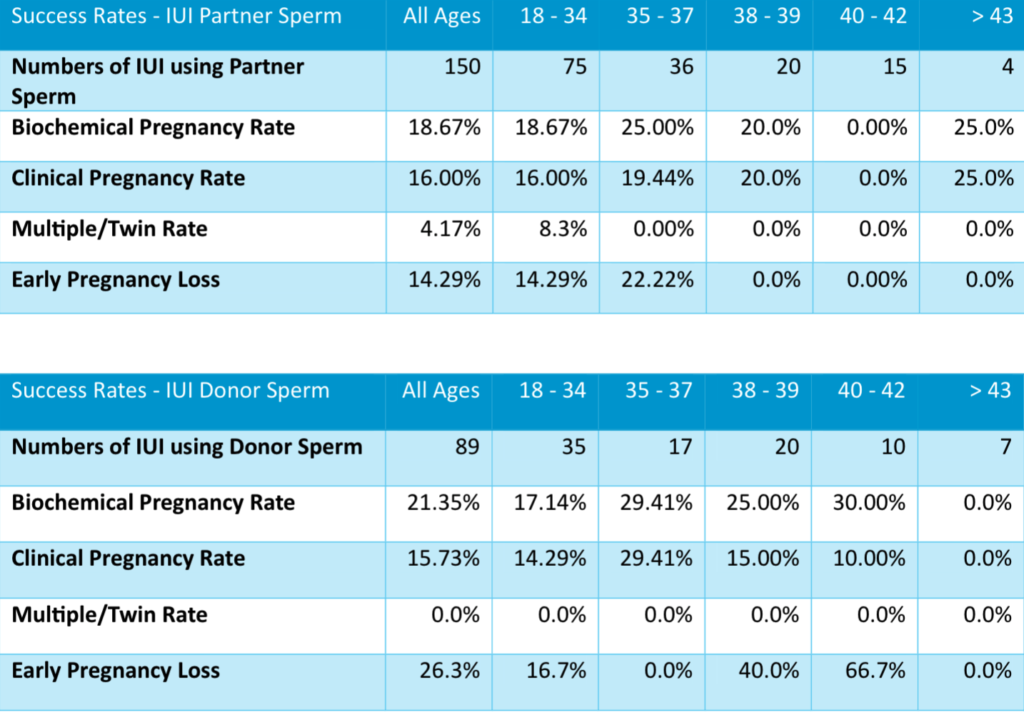
Treatments IUI
Intrauterine Insemination (IUI) is a simpler treatment where sperm is placed directly into the womb. We use either partner or donor sperm.
Sperm quality will dictate whether this is appropriate for your treatment.
Supporting your Fertility Journey
At King’s Fertility, we prioritize your comfort and success through comprehensive support
services. We provide counselling, financial guidance, and educational resources to assist you throughout the fertility treatment process.
Our commitment to excellence in patient care ensures that you receive the utmost attention and support at every step of your journey. We believe in creating a supportive environment where you can feel secure and informed while making important decisions about your treatment options.
Our dedicated staff are always available to address your concerns and provide the necessary resources to help you navigate the fertility process with confidence.
King’s Fertility is an HFEA licensed clinic and, as required by law, we report all our treatment and outcome data to the Human Fertilisation and Embryology Authority, which uses this information in its national statistics and “Choose a fertility clinic” function. While we publish our own success rates to be transparent about our outcomes, it is important to understand that success-rate figures are of limited value when comparing centres or deciding where to have treatment, as they do not take into account your individual circumstances or the complexity of cases treated at different clinics.
We therefore strongly encourage you to view our results alongside the HFEA’s independent information and advice on choosing a clinic, available via the HFEA “Choose a fertility clinic” website (HFEA Choose a Clinic), and to discuss your personal chances of success with a member of our clinical team at your consultation.